Dysplastic nevus (atypical nevus, melanoma-dangerous nevus, Clark’s nevus) is a benign pigmented skin neoplasm with a high risk of transformation into a malignant tumor (melanoma). Dysplastic nevus (DN) can occur at any age, but the older the person, the higher the likelihood. Dysplastic nevi can be multiple, which is especially typical for people with multiple congenital nevi, as well as after excessive exposure to the skin with ultraviolet light (artificial or solar). With the same probability, they can appear in both men and women.
Predisposing factors
There is no clear reason for the appearance of dysplastic nevi. It is only appropriate to talk about predisposing factors that, to varying degrees, can increase the risk of neoplasms:
- Genetic factor (heredity): it was found that the appearance of dysplastic nevi can be inherited in an autosomal dominant manner (dysplastic nevi syndrome). However, this is not the only reason, since Dysplastic nevi appear in people without family associations;
- Ultraviolet radiation: artificial or solar ultraviolet leads to faster reproduction of nevoid cells (nevus cells), the production of melanin (pigment, the accumulation of which is noted in the nevus), and also provokes malignant degeneration;
- Hormonal changes: hormonal fluctuations in the body (especially sex hormones, thyroid hormones and adrenal hormones) can affect the appearance of new nevi and the growth of existing ones;
- Ionizing radiation and skin injuries can also provoke the appearance or growth of dysplastic nevi.
Diagnostics
Diagnosis of dysplastic nevi is based on a clinical examination, which includes a routine examination of the formation and dermatoscopy. If you suspect malignant growth, a biopsy can be performed.
Symptoms
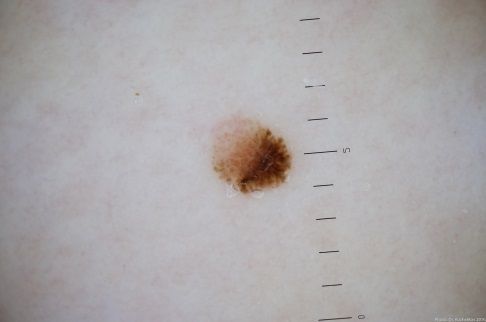
On visual inspection of dysplastic nevus, a spot or slightly elevated nodule is determined. Formation can be either symmetrical (oval, round, elongated), or irregular in shape. The surface of the nevus is a texture of ordinary skin, a smooth skin pattern (up to a glossy surface), small tuberosity, or peeling.
The boundaries of dysplastic nevus are usually fuzzy (blurry), even. Roughness of the edge can be observed, which refers to an unfavorable sign.
The color of the dysplastic nevus is very variable; there may be formations from light brown to dark brown, almost black. Often there are shades of red, pink, blue. The distribution of pigment is usually heterogeneous. This can be a gradual decrease in color intensity in the direction from the center to the periphery, heterogeneity of color over the entire area, spotting (with areas up to the complete absence of pigment), the presence of several colors, or their shades (polychrome).
Hair is most often absent, or a single, sparse growth is noted.
The dimensions of the dysplastic nevus usually do not exceed 10-15 mm, although larger formations (up to several centimeters) can also occur. The growth of dysplastic nevus is often slow. Rapid growth is an unfavorable sign and can mean the transformation of the nevus into melanoma.
On palpation of dysplastic nevus, there are no features: the consistency of ordinary skin. Subjective sensations are absent, sometimes itching is present (especially after the trauma of formation, exposure to ultraviolet light).
There is no typical localization for dysplastic nevi; they can be located in any anatomical region.
Dermatoscopic Description
With dermatoscopy of dysplastic nevus, the following signs are visualized:
- Alternation of light and dark-colored areas of the pigment network;
- Pigment network heterogeneity (atypical pigment network);
- The presence of irregular inclusions of points and globules against the background of the pigment network;
- Globules of various shapes, sizes and colors;
- Asymmetry in color, structure and shape;
- Uneven edges;
- Peripheral radial radiance;
- Polychrome (3 colors);
- The presence of hypopigmentation zones and structureless zones, regression structures.
Differential diagnosis
Differential diagnosis is carried out with such neoplasms as:
- Post-inflammatory hyperpigmentation;
- Congenital dermal melanocytosis;
- Pigmented nevus (simple or papillomatous);
- Hemangioma;
- Blue nevus;
- Spitz Nevus;
- Pigmented basal cell carcinoma;
- Melanoma.
Risks
Dysplastic nevus has a high risk of transformation into melanoma, especially against the background of active ultraviolet radiation (photodamage) or chronic trauma. Signs of a possible malignancy: a change in appearance (active growth, a change in borders, pigmentation), the appearance of subjective sensations.
Tactics
Dysplastic nevus is often almost impossible to distinguish visually from melanoma in situ (the very initial, “zero” stage of melanoma), and therefore such formations in most cases must be removed with a mandatory histological examination.
Dynamic observation is possible only if the dysplastic nevus for a long time does not show signs of activity, and only after examination by an oncologist. The specialist determines the possibility of further dynamic monitoring (terms are determined individually, usually at least 1 time per month) or indications for removal are made.
Removal is also necessary if there is a mechanical damage to the nevus, its active irradiation with ultraviolet or ionizing radiation, if any changes in the nevus itself are noticed or previously absent sensations appear – consultation of an oncologist.
It is necessary to remove those nevi that are subject to constant, chronic trauma to clothing, jewelry, or due to the characteristics of professional employment.
In the case of dynamic observation, photo fixation of skin neoplasms is of great value, which will subsequently determine even minor changes in the appearance of the nevus.
Patients with dysplastic nevi on the skin require an oncologist examination in the spring and autumn (before and after the beach season). Mapping of skin neoplasms is also recommended, which greatly simplifies further observation, the search for new formations, or changes to existing ones.
Treatment
Only surgical (classic, using an electric or radio scalpel) with a mandatory histological examination.
Treatment of dysplastic nevi using destructive methods (laser removal or cryodestruction) is contraindicated.
Prevention
Prevention of the appearance of dysplastic nevi and their malignancy consists in a gentle and careful attitude to the skin:
- Limitation of ultraviolet radiation (tanning bed, solar tanning);
- The use of protective creams during periods of active sun;
- Exclusion of chronic skin trauma;
- Limitation or exclusion of ionizing radiation, occupational hazards;
- Compliance with safety measures when working with skin-damaging factors;
- Personal hygiene and basic awareness of skin tumors.
It also requires regular examination of all nevi, timely consultation of a specialist in the event of external changes, and removal of potentially dangerous neoplasms.