Psoriasis vulgaris, also known as chronic stationary psoriasis or plaque-like psoriasis, is a common chronic inflammatory skin disorder that is scaling on sharply defined red plaques. Often, skin changes are accompanied by itching in combination with changes in the nail plate.
The manifestation of the disease is based, on the one hand, on a polygenic predisposition, on the other, on exogenous and endogenous trigger factors (for example, infections, drugs, mechanical irritation).
The key point in the diagnosis is the clinical picture and the patient’s complaints in conjunction with typical pathognomonic (psoriasis-specific) signs.
The main therapeutic principles include keratolysis (with the help of urea or salicylic acid preparations), as well as a decrease in the inflammatory response and hyperproliferation of keratinocytes (includes local and systemic treatment with various groups of drugs).
Epidemiology
Psoriasis is equally common in both men and women. The approximate distribution is 1-2% of the population. Age does not affect the risk of psoriasis. However, depending on age, psoriasis of the first and second types is distinguished:
- Type I – the onset of morbidity at the age of 20-30 (associated with impaired immune processes that are inherited);
- Type II – onset of morbidity after 50 years (not associated with heredity).
Etiology (causes)
Psoriasis can have a genetic predisposition (hereditary factor), occur against a background of concomitant pathology (more often – autoimmune diseases, anxiety disorders), or be provoked by various triggers:
- Physical effects on the skin;
- Infectious diseases (not only of the skin, but also of internal organs, for example, the upper respiratory tract;
- Taking certain medications: beta-blockers, chloroquine, lithium preparations, interferon;
- Alcohol consumption;
- Unsuitable climate;
- Psychosocial factors: Most often stress.
Clinical picture
Psoriasis is a chronic disease with a recurrent course: periods of exacerbation are replaced by asymptomatic intervals of varying duration.
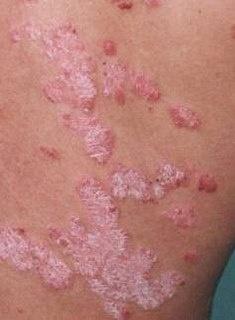
During the period of exacerbation, erythematosquamous plaques appear in the form of sharply outlined redness with underlying skin infiltration and tight-fitting large-lamellar scales of a silvery-white color.
Favorite localization sites for psoriasis:
- The extensor sides of the limbs, especially the elbows and knees;
- Hairy part of the scalp;
- The trunk, especially the sacrum and umbilical region;
- The face, incl. external auditory canal;
- Palms and soles of the feet;
- Genital area;
- Nails: There can be one single pit or many pits. A nail with multiple pits can look like the surface of a thimble, partial and predominantly distal detachment of the nail from the nail bed, the presence of subungual hemorrhages, nail dystrophy in the form of destruction of the nail plate, the appearance of roughness and turbidity.
Itching occurs in about 60% of patients.
Diagnostics
As a rule, the diagnosis of psoriasis is made clinically (by examination).
Physical examination is based on examination and identification of characteristic psoriatic plaques, with the Auspitz psoriatic triad:
- The phenomenon of stearin spot (free discharge of scales from the surface of papules);
- Terminal film phenomenon (reddish shiny surface in the place of removed scales);
- The phenomenon of capillary bleeding (after scraping the red surface, pinpoint bleeding occurs).
In doubtful cases, a biopsy of the affected skin area can be performed for histological confirmation of the diagnosis.
To assess the severity of psoriatic skin lesions, the Psoriasis Area and Severity Index (PASI) is used. This is a system for assessing the area of skin lesions and the severity of the main symptoms. If PASI ≤10 – psoriasis of mild degree, in case of PASI> 10 – a diagnosis of moderate or severe psoriasis is made.
Differential diagnosis
As a rule, the clinical picture of classic (vulgar) psoriasis is quite clear and understandable. However, in certain forms of the disease, such as generalized pustular psoriasis or psoriatic erythroderma, it is necessary to carry out differential diagnosis with diseases such as:
- Lichen planus;
- Atopic eczema;
- Stevens Johnson Syndrome;
- Sézary syndrome;
- Ichthyosiform erythroderma;
- Secondary ichthyosis;
- Bowen’s disease;
- Pink lichen, etc.
Psoriasis treatment
The main goal of treatment for psoriasis is to reduce the severity of symptoms and improve the patient’s quality of life. At PASI ≤10, topical preparations are usually sufficient. When PASI> 10, a combination of local, systemic therapy and physiotherapy is prescribed.
The basic principles of psoriasis therapy include:
- Primary keratolysis as a basic local therapy (preparations containing urea and salicylic acid, moisturizing creams);
- Decreased proliferation activity of keratinocytes;
- Reducing the severity of the inflammatory process on the skin.
As a local treatment, in addition to basic drugs (urea + salicylic acid), calcineurin inhibitors, topical glucocorticoids, calciferol, and retinoids are prescribed.
The indications for the appointment of systemic therapy are:
- Severe psoriasis with a PASI index> 10;
- Psoriatic arthritis;
- Inadequate response to topical or phototherapy.
In this case, retinoids, fumaric acid esters, immunosuppressants, biotherapy (adalimumab, secukinumab, apremilast, etc.) are prescribed. In physiotherapy, phototherapy seems to be the main focus.
Complications
The most frequent complications of psoriasis (usually after a severe and prolonged course) are cardiovascular diseases: hypertension, coronary heart disease, myocardial infarction, acute cerebrovascular accident.
In addition to the effects on the cardiovascular system, metabolic syndrome, obesity and other metabolic problems can occur.
Bacterial infection of psoriasis foci is not typical.
The prognosis for life is favorable, but due to complaints and social stigmatization in patients with psoriasis, the quality of life is significantly reduced.
Prevention
To reduce the risk of developing psoriasis and, to a greater extent, to prevent exacerbations, it is recommended to avoid trigger factors, smoking, excessive alcohol consumption, exclude mechanical skin irritants, monitor body weight, lead a healthy lifestyle (regular physical activity), timely treat concomitant diseases and exclude uncontrolled intake of medicines (without a doctor’s prescription).