Acral nevus (benign nevus of the palms and soles, pigmented nevus of the palms and soles) is a benign skin neoplasm, characterized by its location on the palms and soles. Typically, acral nevus is acquired, but can also be from birth. This type of nevus is not characterized by multiplicity (several acral nevi in one person is rare). Acral nevi make up about 5% of all pigmented nevi.
Predisposing factors
There is no unequivocal cause of acral nevi. It is only appropriate to talk about predisposing factors that may increase the risk of neoplasms to varying degrees:
- Genetic factor: the appearance of acral nevi may be due to the human genome;
- Ultraviolet radiation: artificial or sunlight leads to a faster multiplication of non-void cells (nevus cells) and an excessive production of melanin (pigment, which accumulates in the nevus);
- Hormonal changes: Hormonal fluctuations in the body (especially sex hormones, thyroid hormones and adrenal hormones) can affect the appearance of new nevi and the growth of existing ones;
- Ionizing radiation, viral diseases and injuries can also provoke the appearance or growth of acral nevi.
Diagnosis
The diagnosis of acral nevi is based on clinical examination, which includes a routine examination of the mass and dermatoscopy. A biopsy may be performed if malignant growth is suspected.
Symptoms
Acral nevi are located on the skin of the palms and soles.
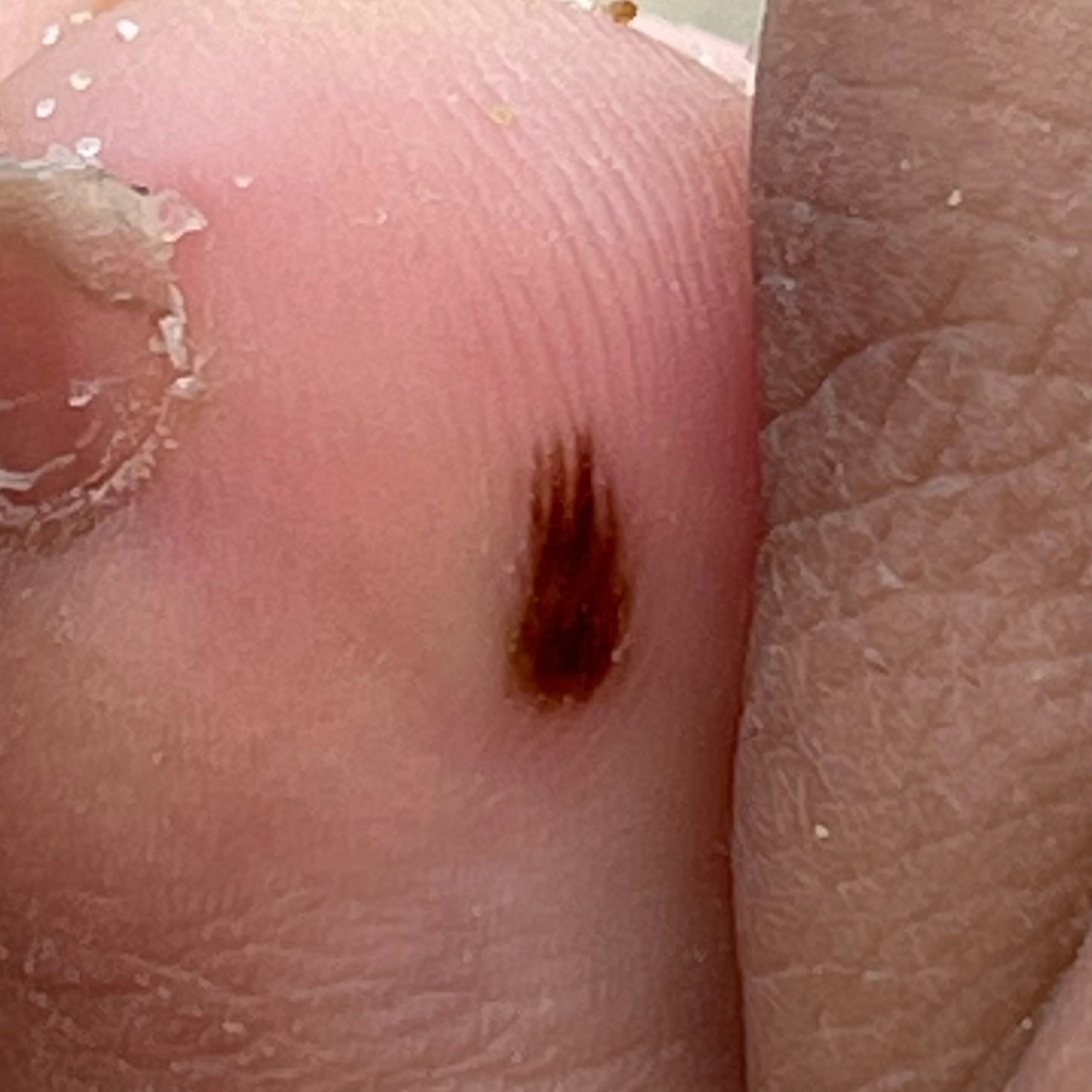
Visual examination of an acral nevus reveals a pigmented neoplasm, most often symmetrical (oval or rounded). The outline is usually irregular due to the presence of a pronounced skin pattern on the palms and soles. The nevus surface does not differ from the texture of normal skin or is slightly fine-browned.
The coloring of acral nevus varies from yellowish brown to dark brown (almost black), with a uniform distribution of pigment throughout the mass. Sometimes there is a gradual decrease in color intensity from the center to the periphery.
The size of acral nevi usually does not exceed 10 mm, most often 3-5 mm. When palpating a simple nevus, there are no peculiarities: the consistency of normal skin. Subjective sensations are also absent.
Dermatoscopic description
On dermatoscopy, an acral nevus is visualized:
- Parallel structure – the linearity of the pattern due to the peculiarities of the skin pattern of the palms and feet;
- Pigment accumulation in the furrows of the skin;
- Lighter pigmentation of the scallops of the skin (pale compared to the furrows);
- The scallops are wider than the grooves;
- Visualization at apex of scallops of sequence from mouths of ducts of perspiratory glands (whitish dots);
- Regular pattern of the above elements (regular sequence of grooves, scallops, mouths).
Differential diagnosis
- Differential diagnosis is made with such pigmented neoplasms as:
- Subcorneal hematoma;
- Contamination of the skin;
- Dysplastic nevus;
- Melanoma.
Risks
An acral nevus is safe and carries no increased risk of melanoma. In the absence of external influence on such a nevus (trauma, ultraviolet light, ionizing radiation), the risk of malignant transformation is comparable to the risk of melanoma in unchanged skin. Signs of possible malignancy: change in appearance, appearance of subjective sensations.
At the same time, the characteristic appearance (heterogeneity of pigmentation, cross-linked appearance, irregular edge) of acral nevus can be very similar to that of melanoma, in particular, acral lentigial melanoma. This is why acral nevi that are
detected for the first time should be of particular concern, in order not to miss an early form of melanoma.
Tactics
In the absence of any damaging effects on the acral nevus, changes in appearance and subjective sensations – self-monitoring (or examination by others in inaccessible areas) at least once a year is sufficient. If there was mechanical damage to the nevus, its active exposure to ultraviolet or ionizing radiation, as well as if you notice any changes in the nevus itself or appeared missing sensations – you need to consult a dermatologist or oncologist.
A specialist determines the possibility of further dynamic monitoring (timing is determined individually), or indications are given for removal of the damaged nevus. Nevi should also be removed if they are permanently and chronically traumatized by clothing, jewelry, or occupation.
In the case of dynamic observation, photofixation of the neoplasm of the skin is of great value, which will make it possible to determine even minor changes in the appearance of the nevus in the future.
It is also recommended to make a map of skin neoplasms, which greatly simplifies further observation, search for new formations or change of existing ones.
Treatment
Only surgical (classical, electro- or radioscalpel) with obligatory histological examination.
Treatment of acral pigmented nevi using destructive methods (laser removal or cryosurgery) is not recommended.
Prevention
The prevention of nevi and their malignization is to treat the skin sparingly and gently:
- Limit UV exposure (tanning beds, sun tanning);
- The use of protective creams during periods of active sunshine;
- Exclusion of chronic traumatization of the skin;
- Restriction or exclusion of ionizing radiation, occupational hazards;
- Observe safety precautions when working with skin damaging factors;
- Personal hygiene and basic awareness of skin neoplasms.
Regular examination of acral nevi, timely consultation with a specialist when external changes occur, and removal of potentially dangerous neoplasms are also necessary.